Congenital Talipes Equinovarus Varus (CTEV)
Commonly Known As, CLUBFOOT.
Introduction
Congenital Talipes Equinovarus Varus (CTEV) commonly known as Clubfoot is one of the most common congenital musculoskeletal deformity among newborns. Although it’s called congenital, it is not an embryonic malformation but is developmental deformation occurring during 2nd trimester.
Incidence:
1:1000
Diagnosis:
It can be diagnosed antenatally during the 2nd trimester of pregnancy during ultrasonography. It can also be identified at birth by the Obstetrician or the neonatologist.
Features:
The Feet are usually inwards (Varus) and downwards (Equinus). It can be Unilateral/ Bilateral, and the severity could vary from mild postural to severe atypical.
Types of Clubfoot:
Typical Clubfoot: Classic Clubfoot and requires Ponseti Protocol of management
Postural/ Positional Clubfoot: Secondary to Intrauterine crowding, its flexible and occasionally needs 1-2 plasters.
Atypical Clubfoot: Subtype wherein the feet are chubby, stiff, short with deep creases and short metatarsals, these are usually difficult to treat and need more expertise.
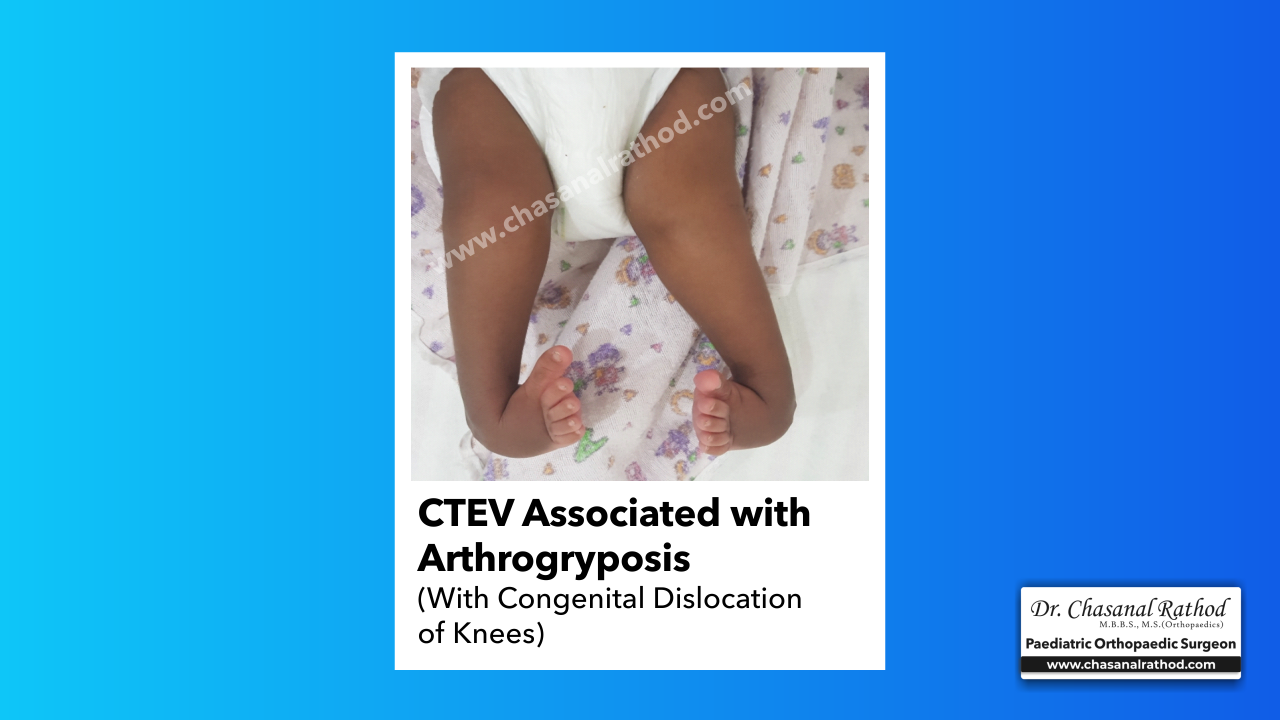
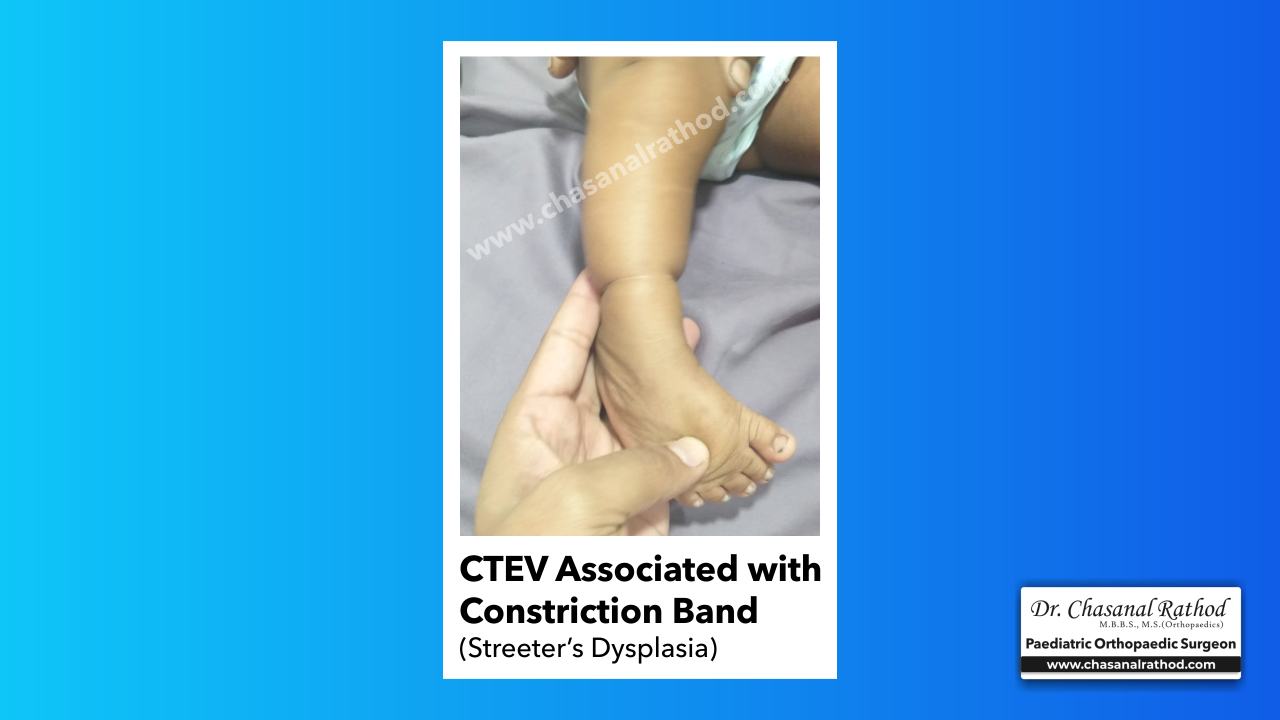
Syndromic Clubfoot: Associated with various syndromes
- Streeter’s dysplasia
- Pierre Robbins Syndrome
- Freeman Sheldon Syndrome
- Arthrogryposis Multiplex congenita
Neurogenic Clubfoot: Associated with spinal dysraphism, myelomeningocele or other neurological condition (HSMN)


Treatment:
The treatment for clubfoot can be summarized depending on the time of presentation.
- Antenatal Diagnosis: Once diagnosed antenatally the family has to be assured that CTEV is fully correctable and the child is capable of having a normal looking foot with essentially normal function. Important is to rule out any spinal involvement or arthrogryposis which make the clubfoot treatment complex and lead to an unfavorable outcome.
- At Birth: Maternal Manipulation: At Birth the mother is advised maternal manipulation of the foot during every feed for 1-2 weeks before the casting begins.
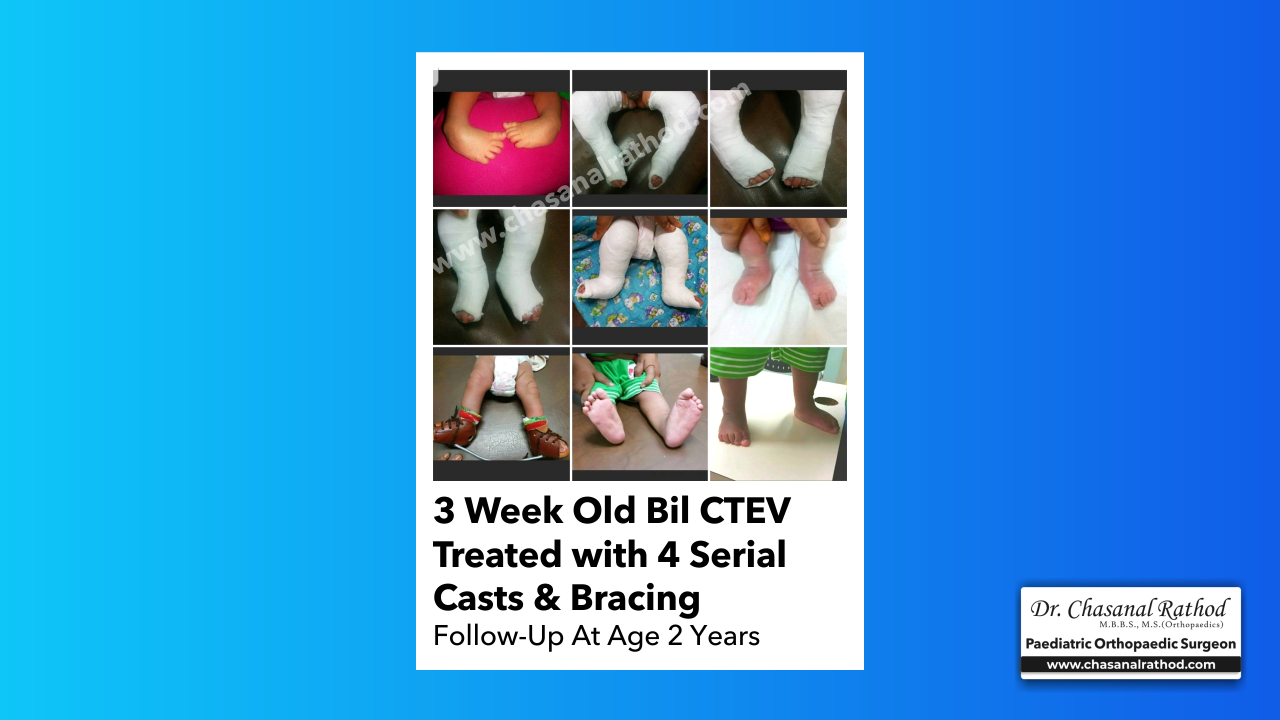
- Infancy: Ponseti Method: The Ponseti Technique is a worldwide accepted and most effective treatment method for clubfoot. The treatment comprises of gradual correction of the deformities (Fig 3) by serial weekly plaster casts. An average 5-7 plasters are required to treat a child with clubfoot presenting in infancy. The older child needs more number of plasters. It is recommended to start plaster cast as early as 2nd or 3rd week after birth, however the higher upper limit as per literature is age 12years which have been treated with this method. After approximately 4-6 casts the cavus , varus and adductus are corrected and 90% of the Clubfeet usually need a mini procedure of Tendoachilles Tenotomy to correct the equinus. This is usually done at the last plaster and this plaster is a 3-weeks duration cast.
Bracing Protocol: The Ponseti treatment along with tenotomy gives excellent results However, a diligent follow up bracing of feet to maintain the foot in abduction and dorsiflexion prevents relapse. The brace comprises of a pair of CTEV shoes in 50-60 deg abduction which are attached to a bar which is curved to maintain the feet in dorsiflexion. The Bracing protocol is 23hrs/day for 3 months and thereafter for naptime and night time till age 4-6 years. - Recurrent/ Relapse CTEV: Weekly manipulations and casts are reinstituted followed by Re-tenotomy and strict bracing. Tendon transfer (Tibialis Ant transfer to realign the soft tissue imbalance are required in some cases.
- Neglected CTEV: Older age group >6years and those who do not respond to non-operative treatment do better with lateral column shortening osteotomy and the more severe ones require gradual correction with fixators (Fig 4) Even after surgery the child needs to wear braces/CTEV shoes/Splints to prevent relapse.Early treatment with Ponseti method and good bracing protocol leads to near normal, supple, pain free feet with good outcome.